
ADHD Medications: Focus, Side Effects, and Maybe Some Sleepless Nights
In my previous post, I explained how an ADHD brain functions and what medication is designed to support. If you haven’t read that yet, I recommend starting there, as it provides helpful context for understanding how these medications work.
Before we zoom in, let’s zoom out for a moment.
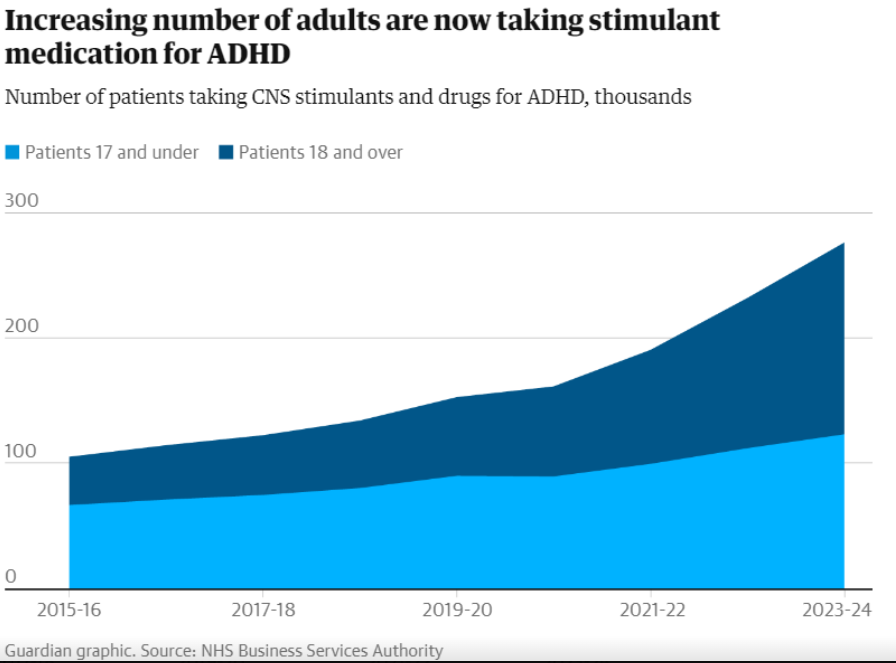
In the UK, around 5 out of every 1,000 people are prescribed central nervous system (CNS) medications for ADHD. Over the past year, prescriptions have increased by 18%, with the majority now being prescribed to women.¹
In this post, we’ll look at:
The most commonly prescribed ADHD medications for children and adults
Broad pros and cons
Key side effects and considerations
Let’s get into it.
Common ADHD Medications
Amphetamine-Based Medications
Adderall
Adderall is an amphetamine-based medication made up of two components: dextroamphetamine (D) and levoamphetamine (L) in a 3:2 ratio.
Dextroamphetamine primarily affects the brain and is more potent
Levoamphetamine has stronger effects on the body, such as increasing heart rate and blood pressure
Adderall works by increasing dopamine and adrenaline activity in the brain. While it may seem counterintuitive to prescribe a stimulant for hyperactivity, the goal is to improve focus and attention by strengthening signalling in specific brain networks.
Vyvanse
Vyvanse is a modified form of dextroamphetamine combined with the amino acid lysine. This design creates a slower release, which can reduce peaks and crashes and lower (but not eliminate) the risk of misuse. The active stimulant component remains strong once metabolised.
Ritalin (Methylphenidate)
Ritalin works on similar pathways to Adderall but has a stronger effect on dopamine than adrenaline. It is generally considered less potent than amphetamine-based medications but is often well tolerated.
Non-Amphetamine Medications
Modafinil
Modafinil is not commonly prescribed for ADHD in the UK and is primarily used for conditions like narcolepsy. It weakly inhibits dopamine reuptake and also increases histamine levels, promoting wakefulness. Its effects on attention can vary significantly between individuals.
Atomoxetine (Strattera)
Atomoxetine is a non-stimulant medication and works as a norepinephrine reuptake inhibitor (NRI). Rather than increasing dopamine directly, it keeps more adrenaline available in the brain, which can help regulate attention and impulse control.
Key Themes to Consider: Pros and Cons
Medication responses are highly individual. Sensitivity, lifestyle, and existing health factors all matter. Below are key themes worth considering rather than a one-size-fits-all verdict.
Sleep Impact
Because ADHD medications affect alertness and energy, sleep disruption is common.
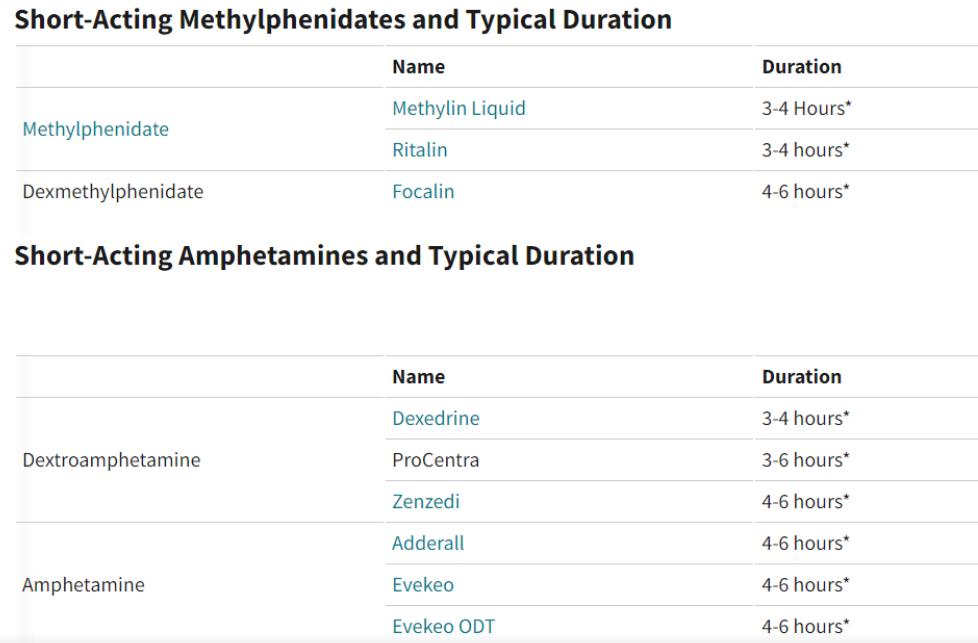
Ritalin is short-acting (around 4 hours), making it a preferred option for those concerned about sleep
Vyvanse is slow-release but can still interfere with sleep in some people
Adderall typically lasts 6–8 hours and may delay sleep onset
Modafinil strongly promotes wakefulness and can severely disrupt sleep if mistimed
Atomoxetine may cause daytime drowsiness, which can indirectly affect sleep cycles
Risk of Dependence
Stimulant medications carry varying degrees of dependency risk.
Adderall has been associated with tolerance and dose escalation in some individuals
Vyvanse was designed to reduce misuse potential, though tolerance can still develop
Ritalin is classified as a Schedule II controlled substance due to abuse potential
Modafinil has a lower addiction risk but can be dangerous when combined with alcohol
Atomoxetine is not classed as addictive, though some people experience reliance on its effects
Dosage and Timing
Finding the right dose and timing is critical for effectiveness and minimising side effects. Each medication has a different active window, and schedules should be tailored to daily demands. Lifestyle factors such as exercise and alcohol use can also influence how medications are tolerated.²
Other Important Considerations
Side Effects
Common side effects across ADHD medications include:
Anxiety
Increased impulsivity
Insomnia
Panic symptoms
Irritability or hostility
More severe effects, such as psychosis, are rare but should be closely monitored, especially in individuals with a personal or family history of mental health conditions.
Long-Term Effects
Long-term research on ADHD medication is still evolving. Much of the existing data focuses on methylphenidate (Ritalin). Some studies suggest prolonged use may influence serotonin activity and cardiovascular health, though findings are still being explored.³
Drug Holidays: Are Breaks Helpful?
There is ongoing debate about whether ADHD medications should be taken daily. Earlier research suggested that “drug holidays” (for example, weekends or school breaks) might reduce side effects. Decisions about breaks should always be made with a healthcare provider, based on individual risks and benefits.
Conclusion
The aim of this post isn’t to push medication for or against, but to provide a clear overview of the ADHD medication landscape.
I feel that the current enviroment leans towards short term gains than long term consequences. Maybe we would be asking different questions.
-Can we provide different external enviroment for students rather than to altering their internal one?
-Is this a permanet solution or a temporary?
-Do adults with ADHD take medication?
I am trying not to say too much here of my own opinion and I am sorry if I have leant more towards the non medication side. I feel that long term consequences are not being looked in more detail. I also think that the pressure of the school enviroment is looking for ways to manage the situation rather than embracing and educating the student.
Medication is one part of the picture. But environment matters too.
I work with children with ADHD online, one-to-one — adapting every session to how they think, what energises them, and what makes them switch off. No box-ticking. No one-size-fits-all.
If your child has ADHD and you're looking for support that works with how their brain is wired, let's talk.
References
The Guardian – NHS ADHD prescription data
https://www.theguardian.com/society/article/2024/jul/26/record-numbers-in-england-taking-adhd-medication-nhs-data-showsADDitude Magazine – Short vs long-acting stimulants
https://www.additudemag.com/short-acting-stimulants-long-acting-stimulants/JAMA Psychiatry – Long-term effects of ADHD medication
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2811812